
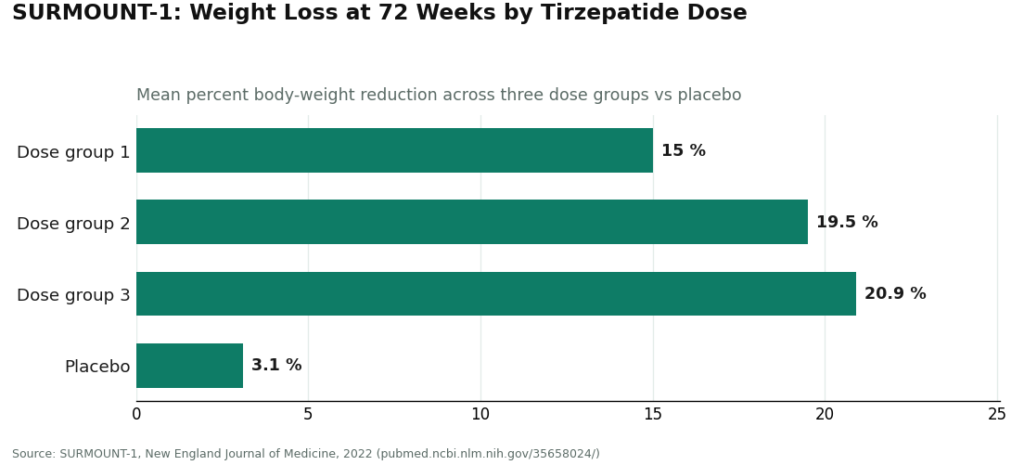
Here is a number I keep coming back to: 72. Not a percentage, not a dose, a length of time. That is how many weeks the SURMOUNT-1 trial ran before it reported its headline tirzepatide results, mean reductions of about 15.0 percent, 19.5 percent, and 20.9 percent across the three dose groups, against 3.1 percent for placebo [1]. Seventy-two weeks is nearly a year and a half. And that single fact, buried in the methods section rather than the marketing copy, tells you almost everything about why so many people feel cheated by peptides in the first month.
I want to lay out an argument here, and it is a simple one once you see it: peptides do not share a timeline, they share a category, and the category tells you nothing about the calendar. Some of these compounds have a documented, week-numbered arc you can hold up to the light. Others have a story that sounds like a timeline but is built from rat cages and forum posts. Confusing the two is where most of the disappointment, and honestly some of the risk, comes from.
The evidence ladder, three rungs
Think of it as a ladder with three rungs, measured in weeks of real human data.
At the top: 72 weeks of controlled trial data for tirzepatide, the kind of evidence that lets a clinician actually tell you what month three should feel like versus month twelve, because the mechanism, slowed gastric emptying, dulled appetite, better glucose handling, is a known, gradual physiological process rather than a mystery [2]. That gradualness is deliberate. Doses are stepped up slowly partly to manage side effects, so a quiet first few weeks is not a failure signal, it is the protocol working.
In the middle, one narrow rung: 12 weeks. That is how long a topical GHK-Cu cream was applied to thigh skin in a study that found roughly 70 percent of the treated women showed improved collagen production [3]. Twelve weeks, real people, real measurement. But it is a cosmetic skin-cream result, and it says nothing about what an injected, whole-body GHK-Cu regimen would do on any schedule. People borrow that 12-week number and apply it to a completely different use case, which is a bit like reading a bus timetable and assuming it tells you when the train leaves.
At the bottom rung: zero. That is effectively where BPC-157 and TB-500 sit. A 2025 systematic review scanned 36 BPC-157 studies and found 35 were preclinical, with a single small clinical study of 12 patients, and it explicitly stated no clinical safety data were found [4]. A separate 2025 narrative review put the total human evidence at three pilot studies [5]. TB-500’s protective effects are documented almost entirely in preclinical work, with human clinical evidence largely absent [6]. There is no rung to stand on. Any “expect results by week four” claim you have read for these compounds was not measured, it was guessed, and then repeated confidently enough that it started to sound like a fact.
The counterpoint I have to give
Now, the honest “but.” You could argue that absence of human trials is not proof of absence of effect, and that is fair as far as it goes. Preclinical signals sometimes do translate to people eventually. Retatrutide is a case in point on the studied side of that fence, a compound still investigational, but with a genuinely promising Phase 2 result on weight loss already published [7]. The gray market has started selling it anyway, ahead of the finished development that would actually earn it a timeline.
But “might eventually work” is a different claim than “here is your week-by-week schedule,” and the second claim is the one being sold. When there is no trial, there is no timeline, full stop. What you have instead is a personal experiment with a sample size of one, no control group, and no one who has done it under measurement to compare notes with. That is a legitimate thing for an adult to choose. It is not the same thing as following a studied protocol, and treating it as equivalent is where the real risk hides, not necessarily in the molecule, but in the false confidence about when and how it should be working.
What this actually means week to week
If you are on a studied medication like semaglutide or tirzepatide, judge yourself on a scale of months, not days. The early weeks are supposed to feel subtle. Save your patience for week twelve, not week two. And keep the labeled risks in view rather than out of mind, semaglutide’s label, for instance, carries a boxed warning for thyroid C-cell tumors and is contraindicated with a personal or family history of medullary thyroid carcinoma [8], which is one more argument for walking this particular timeline with a clinician rather than alone.
If you are experimenting with a research peptide that has no rung on the ladder at all, the honest posture is loose expectations and a sharp eye, because you are generating the only data point that exists. Either way, a simple log, date started, dose, how you actually feel, what changed, does more for your judgment than any promised timeline ever will. It turns a vague feeling into something you and a provider can actually look at together.
Where supervision actually earns its keep
For the studied, prescription, and compounded peptides, this is exactly the terrain where a supervised model like FormBlends does something useful. It is a telehealth platform where a licensed physician evaluates you, a prescription is required, the medication ships from a state-licensed compounding pharmacy, and a care team stays reachable while the slow weeks unfold. I mention it here as an example of what accountable follow-through looks like, not as a product to buy off this page. There is nothing for sale here, just a description of the model.
Supervision will not make a 72-week arc move faster, and it cannot retroactively give BPC-157 the human trials it never had. What it changes is entirely human: someone sets realistic expectations at the start, adjusts the dose as your body responds, and is on the other end of a message during the quiet stretch where you are deciding whether to keep going or bail.
The synthesis
So here is where I land. The number that should anchor your expectations is not some magic “week four” or “week six” you saw on a product page, it is the number of weeks of actual human evidence behind whatever you are taking: 72 for tirzepatide’s headline result, a narrow 12 for topical GHK-Cu, effectively zero for BPC-157 and TB-500. Ask that one question of any peptide before you ask how fast it will work, and the whole conversation gets a lot more honest, including with yourself.
Questions people actually ask
How long do peptides really take to work?
It depends entirely on which one you mean. GLP-1 medications follow a slow, documented arc, the SURMOUNT-1 tirzepatide numbers were measured at 72 weeks [1], so realistically you are looking at months of consistent use, with early changes in appetite and fullness well before the bigger shifts [2]. For most popular research peptides, there is no studied human timeline to hand you, because the human trials mostly were never run [4][5].
Why do the first weeks on a GLP-1 feel like nothing is happening?
Because the dose usually starts low and climbs slowly, partly to keep side effects manageable, and because the underlying effects, slower gastric emptying, reduced appetite, better glucose handling, are gradual biological shifts rather than a switch flipping [2]. Quiet weeks are the mechanism doing its job, not evidence it has stalled.
Is there an actual timeline for BPC-157 or TB-500?
No, not one built on people. What circulates online comes from animal studies and anecdote. A 2025 systematic review of 36 BPC-157 studies found 35 preclinical and reported no clinical safety data found [4], and a narrative review counted only three pilot human studies [5]. TB-500’s evidence in humans is largely absent [6]. Using either compound means you are the study, without a map.
Does GHK-Cu have a real, studied timeline?
A narrow one, yes. A 2018 review documented that a GHK-Cu cream applied to skin for 12 weeks improved collagen production in roughly 70 percent of the women studied [3]. That is a genuine 12-week timeline, but for topical, cosmetic use in a specific trial. It does not license expectations about injected, whole-body effects on any given schedule.
Does going through a supervised provider make peptides work faster?
No. Supervision does not compress a 72-week arc, and it cannot manufacture human trial data for a compound that never had any. What it changes is the experience: a clinician sets sane expectations, adjusts your dose as your body responds, and stays reachable through the slow early stretch. Compounded medications are still not FDA-approved or FDA-reviewed for safety, effectiveness, or quality, so the value supervision adds is judgment and accountability, not speed.
Are companies selling “research use only” peptides actually legitimate?
Some are legitimate suppliers of research materials, but “research use only” sits in a legal gray zone that shifts all the quality and dosing risk onto you. Third-party certificate-of-analysis paperwork varies enormously in reliability, and nobody is routinely auditing these sellers. If you are actually using the product on yourself and want any real safety accountability, a physician-supervised compounding pharmacy, FormBlends among them, operates under a fundamentally different standard.
What does it actually cost to get peptides through a legitimate route?
It swings a lot depending on which peptide, what dose, and how it reaches you. Research-chemical vendors often look cheaper at first glance, but that price rarely covers real purity testing, cold-chain shipping, or any medical oversight. Supervised clinical or compounding routes run higher monthly, but that number is buying consultations, dose adjustments, and accountability a warehouse website simply does not offer.
What should I actually be checking when I compare peptide suppliers?
Start with how quality gets verified. Look for independent, third-party certificates of analysis from an accredited lab, not an in-house PDF. Beyond that, check whether a licensed medical or pharmacy professional is actually involved, how the product is stored and shipped, and whether anyone answers if something goes wrong. A clean website and a low price number tell you almost nothing about what is actually in the vial.
Can I sense whether a peptide is working before I see anything visible?
Sometimes. Deeper sleep, quicker recovery between workouts, less joint soreness, these can show up weeks before anything you can measure on a scale or in a mirror. None of them prove the compound is working, but they are worth tracking. A simple weekly log of sleep, energy, and any side effects gives you and your provider actual data instead of a guess based on how one particular day happened to feel.
References
- SURMOUNT-1 tirzepatide: mean reductions of about 15.0% to 20.9% across doses, measured at 72 weeks, vs 3.1% placebo. “Tirzepatide Once Weekly for the Treatment of Obesity,” New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- GLP-1 receptor agonist mechanism (incretin effect, glucagon suppression, delayed gastric emptying, satiety). StatPearls, NCBI Bookshelf, updated 2024. https://www.ncbi.nlm.nih.gov/books/NBK551568/
- GHK-Cu copper peptide review: about 70% collagen improvement in a 12-week topical skin study; plasma GHK declines with age. International Journal of Molecular Sciences, 2018.
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review,” HSS Journal, 2025.
- Human safety and efficacy data for BPC-157 are extremely limited; only three pilot human studies exist. “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing,” Current Reviews in Musculoskeletal Medicine, 2025.
- Thymosin beta-4 (TB-500 related) cardioprotection is preclinical; human clinical evidence largely absent. “Cardioprotection by Thymosin Beta 4,” Vitamins and Hormones, 2016.
- Retatrutide Phase 2 trial showed meaningful weight loss; the compound remains investigational. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial,” New England Journal of Medicine, 2023.
- Wegovy (semaglutide) label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
Written by Hugo Duarte, health-data reporter. Working from the primary literature cited above. Last reviewed June 2026.
Informational, not clinical advice. Check with a healthcare professional before beginning anything.



